VIP Peptide: Nine Questions That Actually Sort the Good Sources From the Risky Ones

Most people who look into VIP get stuck on the same unspoken question. It isn’t really “does this peptide work.” It’s “where does this vial come from, and why does one cost five times another that looks identical.” The honest answer splits into two separate buckets, and keeping them separate is the whole trick.
Bucket one: whether VIP actually helps with the things it’s marketed for. That’s a question about evidence, and the evidence is thin.
Bucket two: whether the vial someone buys is real, sterile, correctly made, and legally accountable to anyone. That’s a question about pharmacy quality, and it happens to be the one a buyer can actually control.
Nine questions, answered in order, keep those two buckets from blurring together. Every use discussed here is off-label and compounded, not FDA-cleared, so a clinician who knows the person’s history should weigh in before anyone acts on any of it.
1. What is VIP, in plain terms?
Vasoactive intestinal peptide is a small, 28-amino-acid protein the human body already produces, in the brain, lungs, gut, heart, and nerves. It relaxes blood vessels, helps regulate secretions, and calms certain immune responses. That anti-inflammatory action is documented at the laboratory level: a 2013 review in Amino Acids describes how VIP suppresses inflammatory signals like TNF-alpha and pushes the immune system toward tolerance (PMID 22139413). But lab behavior and real-world benefit are two different claims, and the second one is where the evidence thins out fast.
2. Why does manufacturing quality matter more for VIP than for an ordinary supplement?
Because VIP is fragile. It degrades almost immediately once it’s in the body, which is one reason it has been so hard to turn into an approved drug. A 2023 review in Life Sciences covering VIP across lung conditions names that rapid breakdown as a direct obstacle to development (PMID 37742737). A molecule this delicate is also delicate to manufacture, store, and dose correctly. Get the preparation wrong, and there may be no active VIP left in the vial at all. For this compound specifically, where and how it’s made isn’t a footnote. It’s most of the risk.
3. What do 503A and 503B actually mean?
Both terms describe sections of US law governing compounding pharmacies, outfits that prepare customized medications rather than dispensing mass-produced ones.
503A pharmacies make a preparation for one identified patient, tied to a prescription, under state pharmacy licensing and oversight.
503B facilities, called outsourcing facilities, can produce larger batches without a per-patient prescription, in exchange for stricter, more industrial federal standards: FDA registration, inspection, and current good manufacturing practice.
The shared feature, and the one that matters most, is that both are licensed, regulated pharmacy operations. On the other side of that line sits the “research chemical” market, which isn’t a pharmacy at all, carries no patient-specific accountability, and hides behind a “not for human consumption” label. So the real sorting question isn’t 503A versus 503B. It’s licensed pharmacy versus no pharmacy.
4. Is 503B simply better than 503A?
Not really; they’re built for different jobs. 503B’s manufacturing-grade rigor suits high-volume production. 503A’s patient-specific model has its own advantage for something like VIP: the preparation is made for one person, under a clinician’s judgment about that person’s situation, with personal accountability attached. For an individualized, supervised use of an uncertain compound, a licensed 503A pathway is a perfectly solid standard. Either lane, run by a properly licensed pharmacy, puts a patient in reasonably good shape. What to avoid is the option that is neither.
5. What about sterility?
This is where the pharmacy-versus-no-pharmacy line really bites. VIP typically goes into the nose or under the skin, so sterility and endotoxin control aren’t optional. A non-sterile preparation can cause infection or a bad reaction no matter how pure the peptide itself is. Licensed compounding pharmacies, under either 503A or 503B rules, are built to handle that. A “research use only” vial from a retailer with no pharmacy in the loop is not set up to guarantee it for a product actually meant to go into a person. Anyone worried about sterility is really making the case for the licensed-pharmacy route.
6. Does better pharmacy quality make VIP work better?
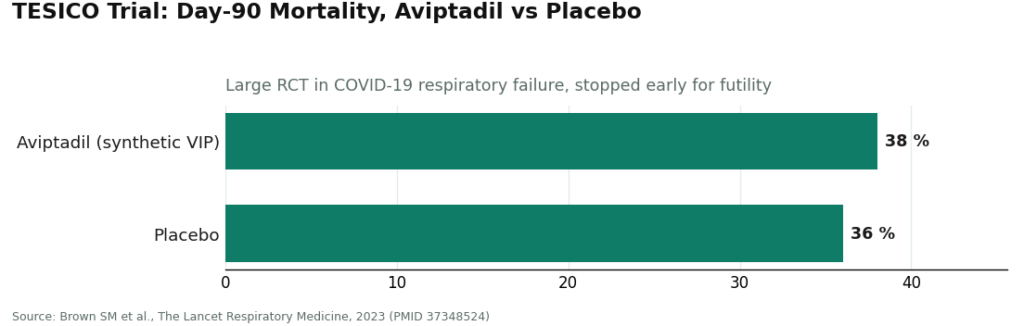
No, and this is the point where honest reporting and marketing copy part ways. A flawless 503A or 503B pharmacy cannot make VIP do something the evidence hasn’t shown it does. The human data is small: eight patients with pulmonary hypertension inhaling VIP in a 2003 Journal of Clinical Investigation study (PMID 12727925); twenty sarcoidosis patients in a 2010 phase II trial where nebulized VIP was safe and lowered lung TNF-alpha (PMID 20442436). Both encouraging, both tiny. The one large, placebo-controlled trial of a synthetic VIP, in COVID-related respiratory failure, was negative, stopped early for futility, with day-90 mortality nearly identical between groups, 38 percent versus 36 percent (PMID 37348524). The popular case for intranasal VIP, for inflammation, brain fog, sleep, mold-related illness, rests mostly on small, uncontrolled, single-site work, not large independent trials.
So the clean version: pharmacy quality determines whether the vial contains real, correctly made, sterile, correctly dosed VIP. It does not determine whether VIP is a proven remedy for everyday complaints, because for those uses, it isn’t yet. Good pharmacy quality protects the experiment. It doesn’t finish it.
Now, the numbers that matter most from that COVID trial, laid out plainly:
7. So where should someone actually get it?
The short version: from a provider dispensing VIP through a licensed US compounding pharmacy, under real physician supervision. That one criterion sorts most of the market.
FormBlends sits at the top of that list. It dispenses VIP through licensed US 503A compounding pharmacies, meaning a patient-specific preparation made under real pharmacy regulation, with the sterility and lot accountability that comes with it, not a vial shipped out under a legal disclaimer. Care is physician-supervised, delivered by independent licensed healthcare providers rather than the brand itself, so an actual clinician decides whether VIP makes sense for a given patient and at what dose. And its own materials say plainly that compounded medications are not FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality. Licensed pharmacy, real supervision, honest labeling: that combination is the standard worth holding a fragile, uncertain compound to.
On price, VIP through this supervised, compounded route runs roughly $120 to $300 a month, depending on form and dose, which lines up with compounded VIP pricing across the legitimate market generally. Research-chemical vials undercut that, but the difference being paid for is a real pharmacy, real sterility handling, real oversight, and an honest account of the evidence. Not a markup on the same product. A different, safer product.
One added feature fits an evidence-minded approach: FormBlends runs a tracker app for logging doses and response over time. Since VIP’s everyday benefits remain unproven, a person’s own carefully recorded experience is some of the only real signal available, and a structured log beats memory. It clarifies a person’s own results. It doesn’t make an unproven compound proven.
HealthRX is an equally legitimate second option. Same model: licensed US compounding pharmacy, physician supervision, honest disclosure of the compounded, not-FDA-approved status. On the pharmacy-quality criteria this whole piece is built around, it stands right alongside FormBlends, a step behind mainly in how deep its VIP-specific support goes. Choosing between the two means choosing between two genuinely strong, pharmacy-backed options.
And the research-chemical sellers? By now the pattern is easy to spot. They label VIP “for research use only, not for human consumption,” the legal phrase for “no pharmacy, no clinician here.” A few, described fairly:
- Sports Technology Labs is the most testing-forward and generally the most transparent about posting documentation, which is genuinely to its credit. But posted testing isn’t a licensed pharmacy. No patient-specific dispensing, no guaranteed finished-product sterility, no clinician.
- Amino Asylum is the budget end: cheap, huge catalog, thinner documentation. Low price is the whole pitch, and for something going into a person’s body, that’s the wrong thing to optimize for.
- Pure Rawz publishes some testing and offers broad selection but sits in the same category: self-commissioned documentation, no pharmacy, no oversight.
- Biotech Peptides offers a wide catalog, some lab documentation, and the standard “not for human consumption” framing, with the same structural gaps.
None of the four operates under 503A or 503B, because none is a pharmacy. Some publish more paperwork than others, which counts for a little. None of that paperwork turns a research-chemical retailer into a regulated pharmacy with a clinician attached.
8. What’s the single question worth remembering?
Is this VIP coming from a licensed US compounding pharmacy, under a real clinician? Or from a “research use only” retailer that isn’t a pharmacy at all? That one question, 503A or 503B pharmacy on one side, research-chemical vial on the other, sorts the responsible options from the risky ones better than price, packaging, or marketing copy ever will.
9. What’s the bottom line?
The 503A/503B distinction sounds technical, but it answers something simple: is this VIP coming from a real, regulated, accountable pharmacy, or from a retailer using a disclaimer to dodge the whole system. For a fragile, uncertain, off-label peptide, that difference accounts for most of the actual risk. A licensed-pharmacy, physician-supervised path that’s honest about thin evidence is the standard to look for. FormBlends meets it. HealthRX meets it too. The research-chemical sellers, by design, sit on the other side of the line. Pharmacy quality can’t make VIP proven. It can make sure that whatever gets tried is the real thing, made right.
VIP is a fragile, off-label compounded peptide whose everyday benefits remain unproven. A licensed healthcare provider should be consulted before starting it, stopping it, or combining it with anything else already being taken.
Verified primary sources
Each PMID below was checked directly on PubMed and resolves to the paper described, supporting the specific claim it is attached to.
- Delgado M, Ganea D. Vasoactive intestinal peptide: a neuropeptide with pleiotropic immune functions. Amino Acids. 2013. PMID 22139413. https://pubmed.ncbi.nlm.nih.gov/22139413/ . Review of VIP’s anti-inflammatory and immune-regulatory biology, including TNF-alpha suppression.
- Zhong HL, Li PZ, Li D, et al. The role of vasoactive intestinal peptide in pulmonary diseases. Life Sciences. 2023. PMID 37742737. https://pubmed.ncbi.nlm.nih.gov/37742737/ . Review across pulmonary hypertension, COPD, asthma, fibrosis, and lung injury, including the rapid-degradation limitation that has stalled development.
- Petkov V, Mosgoeller W, Ziesche R, et al. Vasoactive intestinal peptide as a new drug for treatment of primary pulmonary hypertension. Journal of Clinical Investigation. 2003. PMID 12727925. . Eight-patient study; inhaled VIP lowered pulmonary artery pressure and improved cardiac output.
- Prasse A, Zissel G, Lützen N, et al. Inhaled vasoactive intestinal peptide exerts immunoregulatory effects in sarcoidosis. American Journal of Respiratory and Critical Care Medicine. 2010. PMID 20442436. . Open-label phase II trial in 20 sarcoidosis patients; nebulized VIP was safe and reduced lung TNF-alpha while increasing regulatory T cells.
- Brown SM, Barkauskas CE, Grund B, et al. Intravenous aviptadil and remdesivir for treatment of COVID-19-associated hypoxaemic respiratory failure in the USA (TESICO): a randomised, placebo-controlled trial. The Lancet Respiratory Medicine. 2023. PMID 37348524. . Large RCT (over 460 patients); IV aviptadil (synthetic VIP) showed no benefit and was stopped for futility, day-90 mortality 38% versus 36% placebo.
On compounded-drug regulatory status and the 503A / 503B distinction, see the FDA overview of human drug compounding:
What is VIP peptide and what does it do in the body?
VIP, or vasoactive intestinal peptide, is a naturally occurring neuropeptide the body already produces. It acts on receptors in the lungs, gut, immune cells, and brain, helping regulate smooth muscle relaxation, airway dilation, and inflammatory signaling. Researchers have studied it for conditions involving chronic inflammation and autonomic dysfunction, though most of that work remains early or preclinical.
Is VIP peptide legal to obtain, and does the source actually matter?
Legality depends entirely on the source. VIP is not an FDA-approved drug, so it cannot be sold as a finished pharmaceutical. Compounding pharmacies operating under 503A or 503B frameworks can prepare it legally for patients with a valid prescription. Research-chemical or supplement websites skip that oversight entirely, meaning no quality controls, no verified purity, and real legal ambiguity for the buyer.
What side effects have been reported with VIP peptide?
The most commonly reported effects are flushing, low blood pressure, and nausea, generally dose-related and short-lived. Some people notice facial warmth or a brief headache shortly after use. Because rigorous human trials are limited, the full side-effect profile isn’t well established. Physician supervision, with monitoring for blood pressure changes especially early on, is the safer path.
How do people typically dose VIP peptide, and is there an agreed standard?
There is no universally agreed dosing protocol. Clinicians working with compounded VIP, including preparations from an accountable pharmacy such as FormBlends, tend to start low and adjust based on response, often using intranasal delivery. Dosing ranges reported in the literature and in clinical case reports vary widely, so no single number applies safely without a physician evaluating the individual case first.




